Acute Myeloid Leukemia: Putting Light on FLT3 Mutation
Acute myeloid leukemia (AML) is a phenotypically and genetically heterogeneous but aggressive disease. Major progress has been made to understand mechanisms of leukemogenesis in AML.


Introduction
Acute myeloid leukemia (AML) is a phenotypically and genetically heterogeneous but aggressive disease. Major progress has been made to understand mechanisms of leukemogenesis in AML.
Leukemic Stem Cells and the Two-Hit Model
One of the most relevant hypothesis is the implication of a primitive hematopoietic stem cell or progenitor cell capable of transformation in a so-called leukemic stem cell (LSC), which keeps the ability to self-renewal. This LSC comes from the accumulation of genomic alterations affecting proliferation, cell death and the perturbation of genes involved in the carefully regulated pathways of hematopoietic differentiation. These key oncogenic events are often divided into two classes according to the two-hit model hypothesis of leukemogenesis, in which class I mutations (such as FLT3-ITD) confer a proliferation or survival advantage to blast cells, while class II mutations block myeloid differentiation and give self-renewability. Such events have now been observed in different types of AML.

Genetic Alterations Affecting Differentiation
Differentiation blocks can occur by alteration at specific stages like mutations of CEBPA gene or of the core-binding factor (CBF) complex genes, including RUNX1, which results in different subtypes of AML. The two-hit model of leukemogenesis, combining an activating lesion of tyrosine kinase pathways with an event blocking myeloid differentiation, appears very interesting not only to modelize in vitro leukemogenesis, but also to screen molecular events in AML patients, as observed by the frequent association of an FLT3-ITD mutation with a fusion transcript like AML1-ETO or PML-RARA. Over the past years, besides deregulation of myeloid differentiation resulting from the expression of chimeric proteins, numerous gene mutations have been reported in different types of AML.
FLT3: Structure, Expression, and Function
The FMS-like tyrosine kinase 3 (FLT3) gene, located on chromosome 13q12, encodes a membrane-bound receptor tyrosine kinase (RTK) that belongs to the RTK subclass III family, characterized by five immunoglobulin-like extracellular domains, a single transmembrane domain, a juxtamembrane domain (JMD) and an intracellular domain consisting of two protein tyrosine kinase (PTK) domains linked by a kinase-insert domain. Other members of the RTK subclass III include macrophage colony-stimulating factor (M-CSF) receptor, c-KIT and the receptors for platelet-derived growth factors A and B (PDGFRA and PDGFRB). (2)
Types of FLT3 Mutations
FLT3 is normally expressed by myeloid and lymphoid progenitor cells and expression is lost as hematopoietic cells differentiate. FLT3 plays an important role in the proliferation, differentiation and survival of multipotent stem cells (3) and is overexpressed at the RNA and protein level in AML blasts.(4) FLT3 is one of the most frequent somatic alterations in AML, found in 25–45% of all AML patients.
FLT3 mutations consist of two major types.
- The most common type is an intern tandem duplication (ITD) in exons 14 and 15 (previously known as exons 11 and 12) that map to the JMD, seen in 25–35% of adult and 12% of childhood AML. These ITD, and deletion or insertion/deletion mutations affecting the JMD, are sometimes called length mutations (LM) in the literature. Here, we use the term ITD to refer to all JMD mutations. The length of the duplicated JMD region varies from 3 to 400 nucleotides but, despite this heterogeneity, the resultant transcripts are always in-frame.
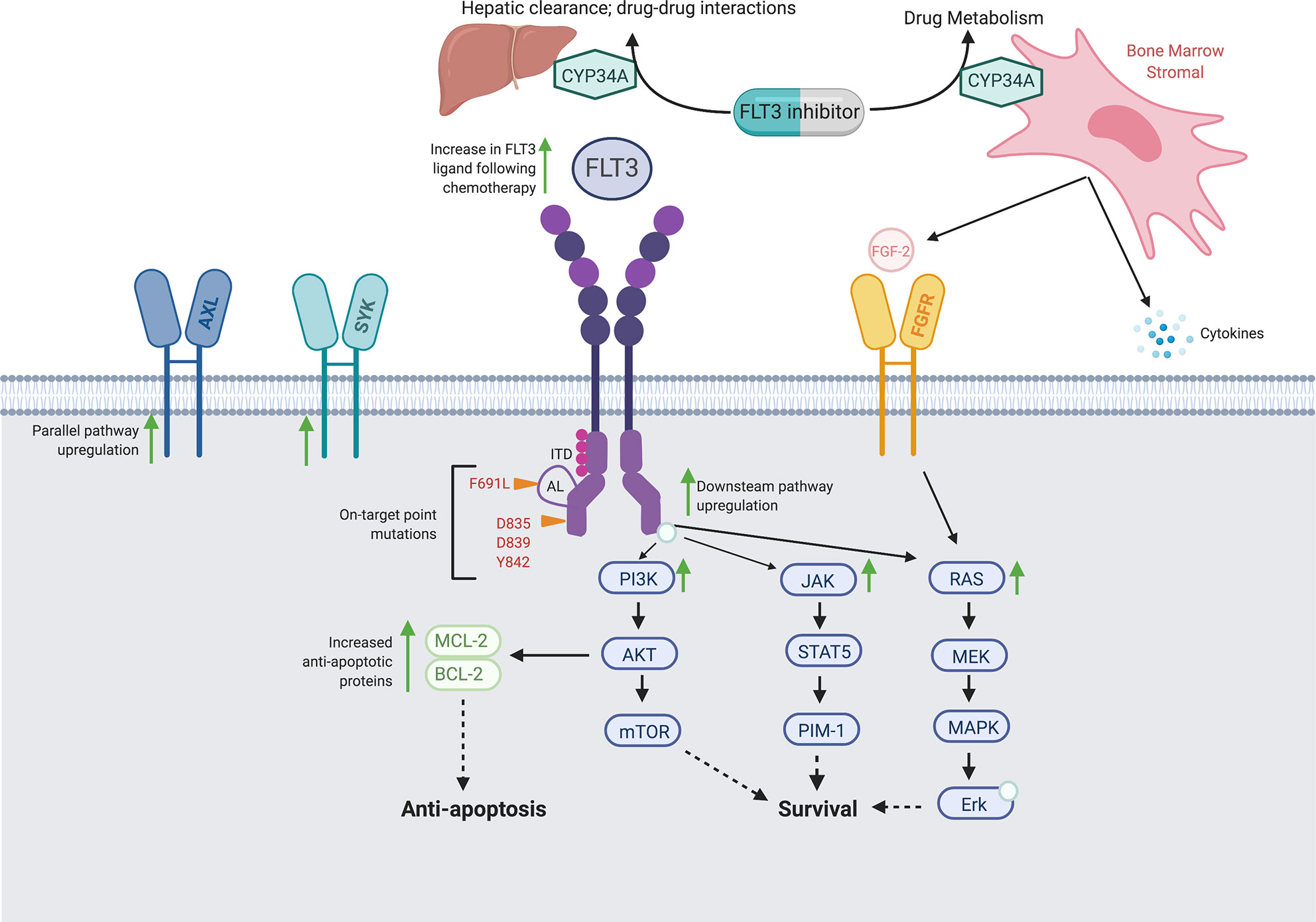
- The second most common type of FLT3 mutation is a missense point mutation in exon 20, within the activation loop (AL) of the tyrosine kinase domain (TKD), found in 5–10% of AML patients. This mutation typically involves codons D835 and/or I836, and less frequently N841 or Y842.18
Several point mutations in the JMD have also recently been described in some AML cases. Their prevalence seems to be lower than 1% in all AML subtypes and has not yet been established in cytogenetically normal AML (CN-AML).Lastly, a novel gain-of-function mutation (K663Q), located not in the AL but in the N-terminal part of TKD, has been recently identified in AML.
Interestingly, a recent study stressed the importance of functional studies, since among the different FLT3 mutations reported outside the JMD and the TKD, some were not associated with kinase activation, and did not contribute to leukemogenesis. Most affected AML patients have only one type of FLT3 mutation, but some patients have both an ITD and TKD of FLT3. FLT3 mutations lead to constitutive phosphorylation of the receptor in the absence of FLT3 ligand and consecutive activation of the downstream signaling pathways such as phosphatidylinositol 3 kinase/AKT, Ras/mitogen-activated protein kinase (MAPK) and Janus kinase 2 (JAK2)/STAT5.However, there is increasing evidence suggesting that the downstream cellular responses to FLT3-ITD and FLT3-TKD mutation are not equivalent.

Clinical Implications and Prognostic Significance
In murine bone marrow transplantation models as well as in transgenic mice, FLT3-ITD induces a myeloproliferative disease that closely resembles human chronic myelomonocytic leukemia, and FLT3-TKD an oligoclonal lymphoid disorder with longest latency, but neither FLT3-ITD nor FLT3-TDK mutations induce AML. These findings support the idea that FLT3 alterations are not sufficient to cause AML. Furthermore, the fact that FLT3 mutations can be acquired or lost at relapse or during disease progression is in accordance with the hypothesis that FLT3 mutations are secondary events in leukemogenesis. The frequency of FLT3-ITD mutations varies dramatically across cytogenetically and molecularly defined subsets of AML. FLT3-ITD has a particularly high incidence in CN-AML and positive AML (30–35% of cases in each group), and in AML. FLT3-ITD-positive patients are more often diagnosed with de novo than secondary AML. Both FLT3-ITD and -TKD mutations have been strongly associated with high white blood cell (WBC) count and high bone marrow blast percentages at presentation. A positive correlation between MLL (mixed lineage leukemia) intragenic abnormalities (MLL partial tandem duplication (MLL-PTD) or DNA double-strand breakage within the MLL breakpoint cluster region induced by topoisomerase II inhibitors) and FLT3 mutations (ITD and TKD) has been reported. In contrast, there is an almost mutually exclusive occurrence of FLT3 and RAS mutations in AML samples. Many studies have shown that FLT3-ITD has a negative impact on outcome in both adult and pediatric AML patients. FLT3-ITD confers a poor prognosis due to an increased relapse rate, reduced disease-free survival (DFS) and overall survival (OS), while the rate of complete remission (CR) is not significantly affected.Several studies restricted to CN-AML have demonstrated that patients harboring at least one allele with FLT3-ITD had a significantly shorter CR duration (CRD), and OS than patients without FLT3-ITD.
Moreover, FLT3-ITD has been found to be an independent prognostic factor for OS, and CRD in CN-AML. However, in other cytogenetic subsets including AML, FLT3-ITD appears not to be an independent prognostic factor.The molecular characteristics of FLT3-ITD are extremely variable among patients. FLT3-ITDs are found in the heterozygous state, but they are sometimes found in a homozygous state after loss of the normal FLT3 allele. A particularly bad prognostic subgroup consists of patients who have lost the wildtype (WT) allele of FLT3. Among intermediate-risk AML, patients with low allelic ratio quantified by Genescan analysis (mutated/WT FLT3o0.8) appear to have survival comparable to AML patients without FLT3-ITD mutations.
The absence of FLT3 WT allele likely results from acquired uniparental disomy, which could be either partial, due to somatic recombination between homologous chromosomes occurring after FLT3-ITD had been generated, or could involve loss of the entire chromosome 13 with the WT allele and subsequent duplication of the remaining homologous chromosome 13 with FLT3- ITD.Another explanation to the variation of allelic ratios lies in the fact that FLT3-ITD may occur only in a subclone of malignant cells and not in LSC. Differences in the size of the duplicated insert may also explain some of the prognostic variability of FLT3-ITDs. A recent study found that patients with larger duplicated segment (over 40 nucleotides) had worse DFS and OS than patients with smaller ITDs.However, this finding was not confirmed by others and needs to be tested on larger cohorts of patients. In contrast to FLT3-ITD, the prognostic impact of TKD point mutations of FLT3 is still controversial. According to a recent study, the impact of FLT3-TKD mutations on OS when including all mutant-positive patients was not significant, but patients with high-level mutations (more than 25% mutant) had significantly improved outcome.30 Further studies are however necessary to determine the clinical relevance of FLT3-TKD, especially in relation with other molecular prognostic factors. FLT3 mutational status may change between diagnosis and relapse, with about 9% (4–27%) of patients losing their FLT3- ITD mutation at relapse, whereas approximately 6% acquire FLT3-ITD mutation on this occasion.
Moreover, in about 6% of FLT3-ITD-positive patients, the length or number of FLT3-ITD change at relapse. The situation is very different for FLT3- TDK mutations, which are lost at relapse in more than 50% of cases. This again strongly suggests that FLT3 alterations are secondary genetic events, occurring in a subclone and not in the LSC. In addition to be a prognostic marker, FLT3-ITD is a potential target for minimal residual disease (MRD) monitoring and for the development of novel treatments
References
- Kondo M, Horibe K, Takahashi Y, Matsumoto K, Fukuda M, Inaba J et al. Prognostic value of internal tandem duplication of the FLT3 gene in childhood acute myelogenous leukemia. Med Pediatr Oncol 1999; 33: 525–529.
- Zwaan ChM, Meshinchi S, Radich JP, Veerman AJ, Huismans DR, Munske L et al. FLT3 internal tandem duplication in 234 children with acute myeloid leukemia (AML): prognostic significance and relation to cellular drug resistance. Blood 2003; 102: 2387–2394
- Meshinchi S, Woods WG, Stirewalt DL, Sweetser DA, Buckley JD, Tjoa TK et al. Prevalence and prognostic significance of Flt3 internal tandem duplication in pediatric acute myeloid leukaemia. Blood 2001; 97: 89–94.