Bangladesh and its Sociology of Medical Knowledge: A Foucauldian Analysis
There has never been a more relevant moment than now to discuss the correspondence between the academic learning on health and its synchronization in the society.

In times like this, the composition of the system of regulation and the structure of the pedagogy with regards to its reception in the crowd appears at its most intricate form. Phrases such as 'social distancing', 'self-isolation' etc. are supposed to be a subject to sociological scrutiny as much as these are of physiology. The imposition of instructions associated with this form of phenomenon ensuing in an effective outcome involves a multidimensional process on the basis of the context in relation to the nature of the mass. And as far as it is the case for Bangladesh, the circumstances are still questionable with a dire need of causative details and leads toward an inspection of the past.
Though the western bio-medicine is recognized as the mainstream medical practice in the developing countries all around the world and Bangladesh as well, simultaneously, the prevalence of the different form of healthcare systems and its acceptability is also noticeable. Unani and Ayurvedic forms of medicament were formally acknowledged by the government of Bangladesh forthwith the war of liberation and were brought under a drug control system in 1982 for further regulation (Bachar, 2014). And though the empirical mode of knowledge generation has been institutionalized, still the conventional rituals such as Kalami, Bhandari, Kabiraji form of healing (Haque et al., 2018) seem to flow under the curtain.
The illustration of such medical pluralism – that is ‘the coexistence of medical subsystems’ (Baer, 2018) - impacts in a crucial way on cases like COVID-19 and begs the question its underlying causes to exist in the first place; and in the context of Bangladesh, Michel Foucault (1926-1984), being a historian of ideas, is very instrumental in providing a relevant sociological lens to look into it.
One of the most profound concepts of Foucault is his perception of knowledge in relation with power which he has delivered in almost all of his major works in one way or another. With a vision of studying history effectively, Foucault developed a technique called ‘archaeology’ in ‘An Archaeology of Knowledge’ (1972), which means to look at history as a way of understanding the processes that have led to what we are today. He also used ‘genealogy’ as a level where the grounds of the true and the false come to be distinguished via mechanisms of power. In ‘Madness and Civilization’ (1967), he talked about the distinction between madness and reasonability and how the notion of madness performed as an essential role in the constitution of reason. In ‘The Birth of The Clinic’ (1973), he traced the development of the medical profession and the institution titled ‘clinic’ and critically viewed the doctoral process of examining body – clinical gaze; whereas in the ‘History of Sexuality’ (Vol.1, 1976), he noted that power is not repressive and sexuality is a positive product of power.
Throughout these works, Foucault indicated that society struggles of discourses belonging to specific forms of discipline and discourses with resistance defying individual’s need - in which power relations are shaped. Hegemonic knowledge creates a regime of truth through institutions, experts and individual which shapes the power structure, and reciprocally, it is the knowledge of the powerful that is able to create such texts with mandates.
A proper image of his view on the respective theme emerged through a discussion entitled as ‘The Politics of Health in the Eighteenth Century’ which got incorporated in the ‘Power/Knowledge: Selected Interviews and Other Writings 1972-1977’, edited by Colin Gordon in 1980. In the very first instance, he stated:
‘Private’ and ‘socialized’ medicine, in their reciprocal support and opposition, both derive from a common global strategy. No doubt there is no society which does not practice some kind of ‘noso-politics’ (p. 166-167).
Furthermore, referring to this politics of disease, he tended to find out the agents as mentioned hereafter:
The centre of initiative, organisation and control for this politics should not be located only in the apparatuses of the State. In fact there were a number of distinct health policies, and various different methods for taking charge of medical problems: those of religious groups (the considerable importance, for example, of the Quakers and the various dissenting movements in England); those of charitable and benevolent associations, ranging from the parish bureaux to the philanthropic societies, which operated somewhat like organs of the surveillance of one class over those others which, precisely because they are less able to defend themselves, are sources of collective danger; those of the learned societies, the eighteenth-century Academies and the early nineteenth-century statistics societies which endeavour to organise a global, quantifiable knowledge of morbid phenomena (p. 167).
To be speculative, in Foucauldian view, the construction of medical knowledge is overridden in diverse manners by the prevailing power structure through its numerous actors in relation to time and space. So, to go further, the history of power circulation on the Bay of Bengal is better to be reviewed.
Geographically Bangladesh had less touch up with the entire Indus civilization. Kola, Bhil, Shabara, Pulinda, Dome, Hadi and Chandal – these present-day ethnic communities are the source for social anthropologists to get access to the ancient society of Bengal (Mazumder, 2010). The tools for agriculture and warfare found in Undivided Bengal dates back to 20,000 years earlier (Sarkar, 2008). These people had no scripts or texts developed by themselves. As a matter of fact, their religion and literature was based on day-to-day practice and very much localized. In times, with the arrival of Aryan here on or about 6,000 B.C.E. (Naidu, 1999), the community-based practices turned into textual and scripted form and often regarded as Vedic tradition. And since the invasion of Aryan, political power construction was never stable in Bengal. Only in the history of Common Era (CE) – Morya, Gupta, Pala, Sen principalities, Sultanate established by Turks, Abbassias, Mamluks, Afghans, Mughals and then as the colony of British as well as Pakistan to a certain extent – Bengal circulated in their hands for almost the last 2,000 years(Murshid, 2016).
Now, the earliest scripture of medical sciences in this subcontinent is found to be the Rigveda and later Ayurveda, developed from the Vedic concept of life (Ghani and Pasha, 2015) that is derived basically from the Aryans whereas Unani has its roots in Greece and developed by the Arabs and spread across this region around 12-13 century CE with the establishment of Delhi Sultanate (1206-1527 CE) and Muslim rule over North India and subsequently flourished under Mughal Empire and the Khiljis (Rogers, 2012). But through the colonization by the British, the celebrated authorities like Atreya, Charaka, Susrata and Vagbhatt were challenged by the new power structure. An apprenticeship model of education was formed, and in time, the old model of ‘basic science education’ and the rapidly generated new information have been in a constant contest here (Sayeed, 2010).
The presented facts depict a specific pattern regarding the construction of medical knowledge in Bangladesh with particular reference toward the power structure relating to the timeframe.
The legal acknowledgement of Unani and Ayurveda in parallel with the modern medicament depicts the exact form of what ‘medical pluralism’ stands for. But each of these genres has been imposed by the invaders – the Aryans, to be specific, the Greco-Roman, Slavo-Germanic and Semitic. On the other hand, the indigenous form of healthcare in relation to various local rituals prevails until now (Haque et al. 2018). People find it reliable whereas the scriptural knowledge has developed before the Common Era.
The underlying cause behind this trend can be the volatility in political power structure which has taken place in the course of history; the frequent swapping among the dynasties led toward the transaction in the official religion of the state, mainstream academia, and favoured learned societies. And thus, no linear form of medical education could be flourished, rather a culture of linsey-woolsey emerged as the time passed.
The outbreak of a pandemic like COVID-19 and the enactments in response to it has also been turned out as very perplexing. Nicholas J. Evans (2020) has talked about social institutions and urban architecture associated with the global pandemic and specified an opinion as follows:
...social distancing differs from other public health measures in terms of the kinds of liberties it infringes upon. Quarantine is the paradigm of a liberty-limiting measure, because it directly and obviously restricts an individual’s freedom of movement in the name of public health.

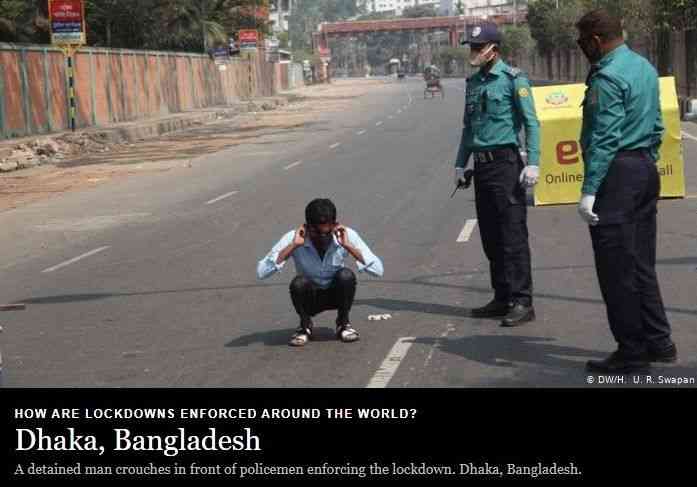
In Bangladesh, the way citizens are reverberating in the retort of the instructions of the medical professionals and the legal operatives, and the way these two institutions are collaborating, reflects a culture that develops as a consequence of suspicion on the fortitude of the entire system. As the authorities in the international scale do not have any strong command over this particular matter, general people have almost no or less regard for the provided information; and the nature of the exercise of power by the state has also triggered a trend among the people to rebuff whenever it is possible. Overall, what the Foucauldian perspective shows us is this unsettling way of life prevailing in this region is a consequence not of an abrupt mania, but of its practices preceding the current context.
Post Image Courtesy: The Financial Express
References:
Bachar, S. C. (2014). Pharmaceutical Industry. Banglapedia: National Encyclopaedia of Bangladesh. Retrieved from http://en.banglapedia.org/index.php?title= Pharmaceutical_Industry on August 31, 2020.
Baer, H. A. (2018). Medical Pluralism. In Callan, H. (Eds.). The International Encyclopedia of Anthropology. John Wily & Sons.
Evans, N. J. (2020). The Ethics of Social Distancing. The Philosopher’s Magazine. Retrieved from https://www.philosophersmag.com/essays/213-the-ethics-of-social-distancing on August 29, 2020.
Foucault, M. (1967). Madness and Civilization: A History of Insanity in the Age of Reason. London: Tavistock.
Foucault, M. (1972). An Archaeology of Knowledge and The Discourse on Language. New York: Pantheon Books.
Foucault, M. (1973). The Birth of the Clinic: An Archaeology of Medical Perception. New York: Pantheon Books.
Foucault, M. (1975). Discipline and Punish: the Birth of the Prison. New York: Pantheon Books.
Foucault, M. (1976). The History of Sexuality Volume 1: An Introduction. London: Allen Lane.
Foucault, M. (1980). The Politics of Health in the Eighteenth Century. In Gordon, C. (Eds.). Power/Knowledge: Selected Interviews and Other Writings 1972-1977 (pp. 166-182). New York: Pantheon Books.
Ghani, A. and Pasha, M. K. (2015). Traditional Medicine. Banglapedia: National Encyclopedia of Bangladesh. Retrieved from http://en.banglapedia.or/index.php? title=Traditional_Medicine on March 27, 2018.
Haque, M. I., Chowdhury, A. B. M. A., Shahjahan, M. & Harun, M. G. D. (2018). Traditional Healing Practices in Rural Bangladesh: A Qualitative Investigation. BMC Complementary and Alternative Medicine. 18(62). pp. 1-15.
Mazumder, S. (2010). Bangladesher Pracheen Shamaj. Dhaka: Bangla Academy.
Murshid, G. (2016). Hajar Bochorer Bangali Sanskriti. Dhaka: Oboshor Prokashon.
Naidu, U. (1999). Bible of Aryan Invasions. Jabalpur: Sudrastan Books.
Rashid, S. (2017). Folk Medicine and Traditional Medical Practices in Bangladesh. The Financial Express. Retrieved from https://thefinancialexpress.com.bd/views/folk-medicine-and-traditional-medical-practices-in-bangladesh on March 27, 2018.
Rogers, K. (2012). Unani Medicine. Encyclopaedia Britannica. Retrieved from https://www.britannica.com/science/Unani-medicine on August 31, 2020.
Sarkar, S. (2008). History of Bengal just got a lot older. The Telegraph: Calcutta. Retrieved from https://www.telegraphindia.com/india/history-of-bengal-just-got-a-lot-older/ on April 12, 2017.
Sayeed, M. A. (2010). Medical Education in Bangladesh - Past, Present and Future. Ibrahim Medical College Journal. 4(2). pp. i-ii.